
INDICATIONS
- Antiretroviral Management in the Newborn:
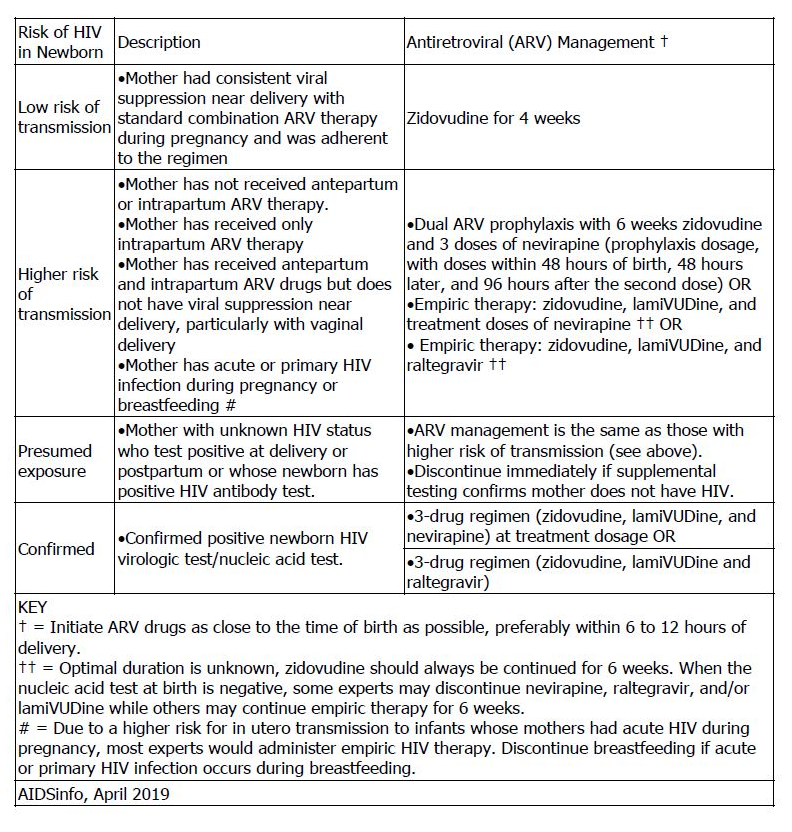
- Prevention of maternal-fetal HIV transmission: In a phase III randomized trial (n=1684), the combination of 6 weeks of zidovudine plus 3 doses of nevirapine or the combination of 6 weeks of zidovudine plus nelfinavir and lamiVUDine for 2 weeks was associated with a lower intrapartum transmission rate when compared with zidovudine alone in infants born to women who received no antenatal antiretroviral therapy (2.2% versus 2.5% versus 4.9%, respectively). The zidovudine/nelfinavir/lamiVUDine regimen was associated with increased toxicity (eg, neutropenia)
PRECAUTIONS
- Coinfection (HIV-1 and hepatitis C virus):
- Hepatic decompensation, some cases fatal, has been reported in patients receiving combination antiretroviral therapy and interferon alfa with or without ribavirin; monitoring recommended; discontinuation of zidovudine or dose reduction or discontinuation of interferon alfa or ribavirin may be required.
- Concomitant Use:
- Avoid concomitant use with doxorubicin or stavudine.
- Concomitant use with ribavirin is not recommended.
- Endocrine & Metabolic:
- Lactic acidosis, including fatal cases, has been reported with nucleoside analog use, including zidovudine; most cases occurred in women and risk factors include female sex and obesity; suspend treatment if suspected.
- Lipoatrophy has been reported and is most evident in the face, limbs, and buttocks; monitoring recommended and use of alternative treatment regimens may be warranted.
- Hematologic:
- Hematologic toxicity, including reports of neutropenia, severe anemia, and pancytopenia have occurred; increased risk with dose and duration of therapy and especially in patients with advanced HIV disease; monitoring recommended; dose adjustments, interruption, discontinuation and/or blood transfusions may be necessary.
- Bone marrow compromise (granulocyte count less than 1000 cells/mm(3) or hemoglobin less than 9.5 g/dL) is associated with an increased risk for hematologic toxicities; monitoring recommended; dose adjustments or discontinuation may be necessary.
- Hepatic:
- Hepatic impairment; increased risk for hematologic toxicities; monitoring recommended.
- Severe hepatomegaly with steatosis, including fatal cases, have been reported with nucleoside analog use, including zidovudine; most cases occurred in women and risk factors include female sex and obesity; suspend treatment if suspected; use with caution in patients with known risk factors for liver disease.
- Immunologic:
- Autoimmune disorders (eg, Graves disease, polymyositis, Guillain-Barré syndrome) have been reported in the setting of immune reconstitution syndrome; onset is variable and may occur several months after treatment initiation.
- Immune reconstitution syndrome has been reported; patients may develop inflammatory response to residual opportunistic infections during initial antiretroviral treatment phase; further evaluation and treatment may be necessary.
- Latex Allergy:
- Zidovudine injection vial stopper contains dry natural rubber latex (a latex derivative) which could cause hypersensitivity reaction in latex-allergic patients.
- Musculoskeletal:
- Symptomatic myopathy and myositis has been associated with prolonged use of zidovudine
- Renal:
- Dose reduction recommended in patients with severe renal impairment (CrCl less than 15 mL/min).
ADVERSE EFFECTS
Anemia and neutropenia occur frequently, and are associated with serum concentrations greater than 3 micromol/L. Mild cases usually respond to a reduction in dose . Severe cases may require cessation of treatment and/or transfusion. Bone marrow toxicity may be increased by concomitant administration of acyclovir, ganciclovir, and sulfamethoxazole/trimethoprim. Transient lactic acidemia is common in infants exposed to in utero highly active antiretroviral therapy or neonatal zidovudine . Concomitant treatment with fluconazole or methadone significantly reduces zidovudine metabolism – dosing interval should be prolonged.
ADMINISTRATION
- Oral:
- Can be given without regard to food.
- Measure syrup with an appropriate-sized syringe with 0.1-mL graduation to ensure accuracy.
- Intravenous:
- Administer IV at a constant rate over 1 hour at a concentration not greater than 4 mg/mL.
- Rapid infusion or bolus injection should be avoided.
- Should not be given intramuscularly.
- Recommended concentration for IV administration is 4 mg/mL.
The National Institute for Occupational Safety and Health (NIOSH) recommends the use of single gloves by anyone handling intact capsules or administering from a unit-dose package . In the preparation of capsules, NIOSH recommends the use of double gloves and a protective gown. Prepare in a ventilated control device, if possible. Use respiratory protection if not prepared in a control device. During administration, wear single gloves, and wear eye/face protection if the formulation is hard to swallow or if the patient may resist, vomit, or spit up . NIOSH recommends the use of double gloves and a protective gown by anyone handling a hazardous oral liquid or any hazardous drug via a feeding tube. Prepare in a control device, if possible. Use respiratory, eye, and face protection if not done in a control device. During administration, eye/face protection is needed if the patient may resist, or if there is potential to vomit or spit up . In the preparation and administration of injections, NIOSH recommends the use of double gloves and a protective gown. Prepare in a biological safety cabinet or a compounding aseptic containment isolator; eye/face and respiratory protection may be needed. Prepare compounds in a closed system drug transfer device. During administration, if there is a potential that the substance could splash or if the patient may resist, use eye/face protection. Administer certain dosage forms via a closed system drug transfer device.
BLACK BOX WARNING
Zidovudine has been associated with hematologic toxicity, including neutropenia and severe anemia, particularly in patients with advanced HIV disease. Prolonged use of zidovudine has been associated with symptomatic myopathy. Lactic acidosis and severe hepatomegaly with steatosis, including fatal cases, have been reported. Suspend treatment if clinical or laboratory findings suggestive of lactic acidosis or pronounced hepatotoxicity occur.
MONITORING
- Prevention of maternal-fetal HIV transmission: Initial Neonatal Management: Obtain a baseline CBC with differential; timing of followup monitoring depends on numerous exposure risks. Recheck hemoglobin and neutrophil counts 4 weeks after initiation of prophylaxis for infants who receive combination zidovudine/lamiVUDine-containing antiretroviral prophylaxis regimens.
- Treatment of HIV infection:
