
INDICATIONS
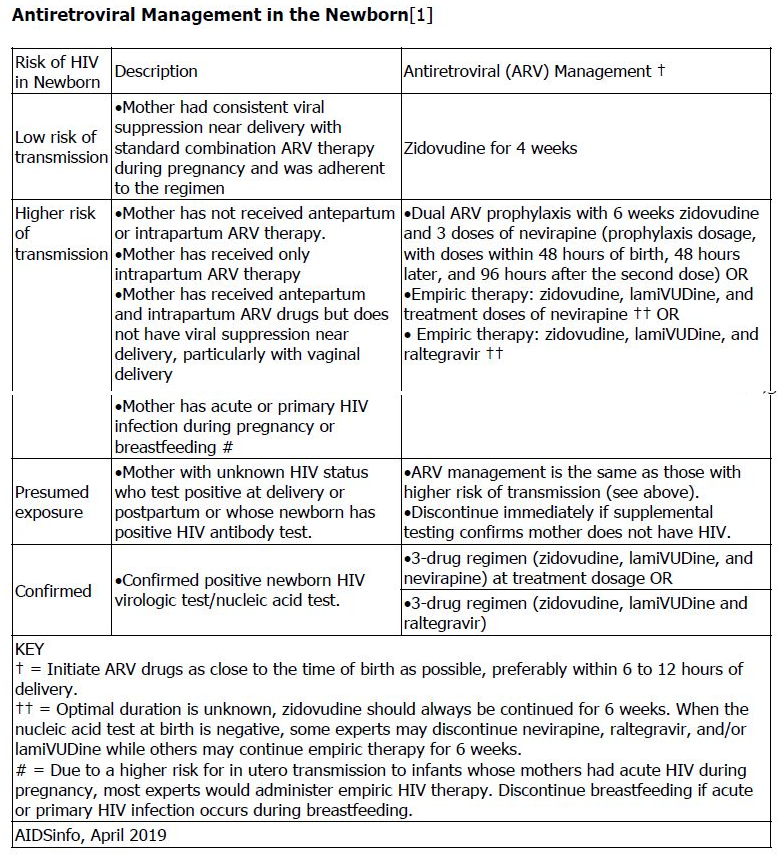
- Antiretroviral Management in the Newborn:
- Prevention of maternal-fetal HIV transmission: . In a phase III randomized trial n=1684), the combination of 6 weeks of zidovudine plus 3 doses of nevirapine or the combination of 6 weeks of zidovudine plus nelfinavir and lamiVUDine for 2 weeks was associated with a lower intrapartum transmission rate when compared with zidovudine alone in infants born to women who received no antenatal antiretroviral therapy (2.2% versus 2.5% versus 4.9%, respectively). The zidovudine/nelfinavir/lamiVUDine regimen was associated with increased toxicity (eg, neutropenia).
FDA APPROVED INDICATION
in combination with other antiretroviral agents as either immediate release tablets or suspension in pediatric patients 15 days or older or extended-release in patients 6 years or older with a body surface area of 1.17 m2 or greater
CONTRAINDICATION
- Neonatal transient myasthenia gravis. Neonatal persistent (congenital) myasthenia gravis.
CONTRAINDICATION
- Hypersensitivity reactions, including severe rash, blisters, oral lesions, conjunctivitis, facial edema, muscle or joint aches, general malaise, and significant hepatic abnormalities have been reported. The risks of hepatic events or skin reactions are greatest in the first 6 weeks of therapy. The hepatic events may occur at any time during therapy. Hepatic injury may progress despite discontinuation of treatment. Children with CD4 percentages greater than 15% are at increased risk for hepatotoxicity and rash at initiation of nevirapine . Immune reconstitution syndrome and fat redistribution may occur. Avoid concomitant use with St. John’s wort-containing products, efavirenz, atazanavir, fosamprenavir (without ritonavir), boceprevir, telaprevir, or another non-nucleoside reverse transcriptase inhibitor
ADVERSE EFFECTS
Limited data on toxicity; none reported in neonates.
Common adverse events in children have been similar to those observed in adults (ie, rash, fever, nausea, headache, diarrhea, abdominal pain, fatigue, and abnormal hepatic transaminases). However, granulocytopenia was more common in children than adults. Hepatotoxicity due to nevirapine appears to be less frequent in children than in adults. In pediatric clinical studies, rash has been reported in up to 27% of patients.Neutropenia (9%), anemia (7%), and hepatotoxicity (2%) have also been reported in children.
ADMINISTRATION
- Can be given without regard to food.
- The National Institute for Occupational Safety and Health (NIOSH) recommends the use of single gloves by anyone handling intact tablets or capsules or administering from a unit-dose package.
- In the preparation of tablets or capsules, including cutting, crushing, or manipulating, or the handling of uncoated tablets, NIOSH recommends the use of double gloves and a protective gown. Prepare in a ventilated control device, if possible. Use respiratory protection if not prepared in a control device. During administration, wear single gloves, and wear eye/face protection if the formulation is hard to swallow or if the patient may resist, vomit, or spit up.
- NIOSH recommends the use of double gloves and a protective gown by anyone handling a hazardous oral liquid or any hazardous drug via a feeding tube. Prepare in a control device, if possible. Use respiratory, eye, and face protection if not done in a control device. During administration, eye/face protection is needed if the patient may resist, or if there is potential to vomit or spit up
BLACK BOX WARNING
Severe, life-threatening, in some cases fatal, hepatotoxicity and skin reactions (eg, Stevens- Johnson syndrome; toxic epidermal necrolysis; and hypersensitivity reactions characterized by rash, constitutional findings, and organ dysfunction) have been reported. Women, including pregnant women, and/or patients with higher CD4+ cell counts are at higher risk of hepatotoxicity. Permanently discontinue nevirapine following severe hepatic, skin, or hypersensitivity reactions. Monitor patients intensively during the first 18 weeks of therapy with nevirapine to detect potentially life-threatening hepatotoxicity or skin reactions. Strictly follow the 14-day lead-in period with immediate-release nevirapine 200 mg daily dosing.
MONITORING
- Initial Neonatal Management:
- Obtain a baseline CBC with differential; timing of followup monitoring depends on numerous exposure risks. Recheck hemoglobin and neutrophil counts 4 weeks after initiation of prophylaxis for infants who receive combination zidovudine/lamiVUDine-containing antiretroviral prophylaxis regimens.
- Perform virologic test at baseline, 14 to 21 days of life, 1 to 2 months of age, and 4 to 6 months of age.
- For nevirapine, frequent monitoring for hepatic toxicity, including liver function tests, during the first 12 weeks of therapy is recommended.
- Check transaminase levels immediately if a patient presents with signs or symptoms indicative of hepatitis and/or a hypersensitivity reaction, or if patient develops rash within first 18 weeks of nevirapine therapy. Permanently discontinue nevirapine in patients with rash-associated transaminase elevations.